BN4410 Health and Safety Management Assignment Sample : Evaluation of the Fukushima Disaster 2011
Here’s the best sample of BN4410 Health and Safety Management Assignment Sample : Evaluation of the Fukushima Disaster 2011, written by the expert.
Introduction
The aim of this report is to provide a case study evaluation of the 2011 Fukushima Meltdown that happened in Japan. The report will take the perspective of the health and safety management appliances that were in place prior to the event and the consequences of the event. The report will also aim to bring to light an evaluation of the said processes and systems and their consequences from an academic perspective. Through this the report will show that the Nuclear Power Plants at Fukushima were designed and monitored based on evaluation of previous plants similar in nature and there was a distinct lack of on-site preparatory processes. The report will also present the relevant health and safety legislations that were put in place and the constraints that they provided to the entire event. The paper is divided into 7 primary sections. The first section provides a background to the entire event, the second section discusses the consequences of the even from a health and safety perspective. The third section details the health and safety concerns in the after math of the event from an academic perspective. The fourth section provides an evaluation of the relevant legislations and regulatory bodies that were responsible for the plant. The fifth section offers a reflective understanding of the recommendations based on the academic papers sourced by the author. The sixth section presents the conclusions that can be drawn from the report and the seventh section presents the appendices for the report.
Background of the event
The Fukushima Disaster, as it is called happened on the 11th of March 2011 when an earthquake, registering 9.0 on the Richter scale, off the coast of Japan caused a tsunami that hit the Tohoku region of Northern Japan. This event resulted in massive damages to persons and property across the region with over twenty thousand people killed or missing. As a result of the earthquake and the tsunami, reactors at the Fukushima nuclear reactors were shut down. However, to maintain the reactors from meltdown, external power was still required which was also disrupted as a result of damages to the infrastructure. The backup power generators were also damaged when the plant was flooded by 14 to 15 meter waves which consequently resulted in the nuclear meltdown at the plant. (Hollnagel & Fujita, 2013)

The immediate result of the core meltdowns at reactor 1, 2 and 3 of the plant was that massive amounts of radioactive materials were released into the environment following the hydrogen explosions. According to a report by the Sasakawa Peace Foundation (TSPF) (2012), it could be reported that radioactive contamination of the atmosphere, soil and the ocean waters had occurred. The report further notes that only 2% of the iodine-131 and 1 per cent of the cesim-137 were released into the environment (TSPF, 2012). This reduced scope of exposure could be one of the reasons that no deaths directly attributable to radiation could be observed from the accident. According to Hasegawa, et al. (2016), most of the deaths from the incident resulted among institutionalised patents and elderly who had to be evacuated from the region.
Consequences of the event
Hasegawa, et al. (2016) noted a comprehensive account of the health consequences of the Fukushima event and the following section is largely drawn from the findings of that report. They (ibid.) note that the fundamental causalities in terms of death cannot be attributed to the radiation exposure by itself, and rather on the management of the evacuation and the emergency response teams. A significant portion of the immediate causes of death were although as a result of drowning in the initial flooding. Hollnagel and Fujita (2012) had noted that there were several systemic failures that led to this initial death toll. They take the resilience abilities of the plants in “responding, monitoring, learning, and anticipating” and find that “inadequate engineering anticipation or risk assessment during the design, in combination with inadequate response capabilities, precipitated the disaster” (Hollnagel and Fujita, 2012). This is also supported by the findings of the IAEA (2014) who also noted that “the regulations, guidelines and procedures in place at the time of the accident were not fully in line with international practice in some key areas, most notably in relation to periodic safety reviews, re-evaluation of hazards, severe accident management and safety culture.” The lack of initial planning in the design and development of the plant and its process was also noted by Ramachandran & Karthikevan (2014) who found that “when the facility of Fukushima Daiichi was constructed, the standards of design were based on historical information only and did not regard the consequences of earthquake and tsunami together.”
Apart from the preliminary shortcomings of the design, development and monitoring phases, Hasegawa, et al. (2016) also find several issues in the disaster response management in the aftermath of the event. They (ibid.) find that the evacuation and relocation plans were mired by insufficient communication on part of the authorities and the government and that evacuation zones were expanded periodically with no concrete protection guidelines being provided to the public. In addition to that, there did not exist any proper evacuation plan for the people. Hasegawa, et al. (2016) also note that “insufficient transportation and disruptions in electricity, water, gas supply, telecommunications and radiation-monitoring systems caused by the earthquake made it more difficult to implement an organised evacuation,” which further bolstered the causalities and damages in the aftermath. In the evacuation of patients and elderly admitted to hospitals, there was an absence of proper toll keeping and information dissemination and on top of that even their transportation was done in non-conducive vehicles for long periods of time without the presence of medical professionals in a lot of the cases (Hasegawa, et al., 2016). They (ibid.) also note as a consequence of the sudden uprooting the health concerns that arose out of living in temporary shelter and the behavioural impact that it had on the affected. There were also other issues like the mental health problems, poor health perceptions and other life-style related problems that arose out of the incident (Hasegawa, et al., 2016). These issues will be discussed in greater detail in the subsequent section of the report.
Health and safety concerns
In regards to the evaluation of the health and safety concerns in the aftermath of the event, there were four primary tools that need to be highlighted – comprehensive medical check – up, mental health and lifestyle, thyroid ultrasounds and pregnant women and nursing mothers (Yamashita, 2016). As noted in previous cases of radiation exposure in Chernobyl and elsewhere, there was a very real chance of the propagation of thyroid cancer especially among children, although it was pretty unlikely given the significantly lower radiation leakage during this event (Yamashita, 2016). Still in order to assuage the fears of the public and to ensure the provision of detailed understanding of the consequences of possible radiation exposure, the government of Japan started screening 370,000 children for signs of radiation induced thyroid cancers. Another important aspect in this regard is that of comprehensive health check-ups for those who were within the evacuation zone. In all, the target population of 210,000 people were provided with comprehensive health check-ups in the month following the event. Yamashita (2016) notes that through this undertaking it was found that, “obesity and hyperlipidaemia exist, even at young ages, and are increased in comparison with the previous years’ data on Fukushima Prefecture in adults of both genders. Liver dysfunction and hyperuricemia increased at relatively young ages in males. Hypertension, glucose dysmetabolism and renal dysfunction increased in adulthood and are most common in older ages.” Again, from the observations in Chernobyl it had been noted that mental health and lifestyle changes were among some of the more pronounced effects of such disasters. The findings of comprehensive surveys in the aftermath of the event revealed that the perception of being exposed to radiation caused greater psychological stress among the evacuees (Hasegawa, et al., 2016; Yamashita, 2016). With regards to maternity and post natal cases it was found that the event did not have any significant health concerns for those affected other than that discussed under the above topics (ibid.). Hasegawa, et al. (2016) also noted several other elements of psychological impacts in the after math of the event including post-traumatic stress responses, chronic anxiety and guilt, ambiguous loss experience, self-stigma and other effects of separated families and communities.
Evaluation of relevant legislations in Japan
The evaluation of the relevant legislations applicable in the scenario in Japan was done based on the report submitted by the Director General of International Atomic Energy Agency (IAEA) (2014), titled ‘The Fukushima Daiichi Accident’. Appendix A provides a detailed summary of the relevant legislations and the responsible authorities. In the framework of safety regulations, the Japanese government had a multiple laws at the central level which each had a number of subordinate acts and ordinances through specific ministries.
The basic regulations included the Atomic Energy Basic Act, Electricity Business Act and Disaster Countermeasures Basic Act. These defined the roles of the authority structure for the various organisations working within the regulatory framework. Under these there were specific ordinances that allowed greater clarity and definition to those acts. Under the Atomic Energy Basic Act, there were subordinates acts namely the Reactor Regulation Act and the Radiation Prevention Act. Similarly under the Disaster Countermeasures Basic Act, there was the subordinate act titled “Act of Special Measures Concerning Nuclear Emergency Preparedness.”
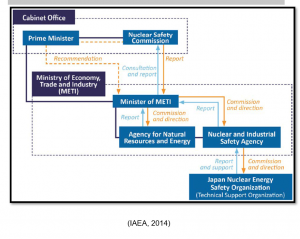
There were several bodies that had the regulatory oversight over various aspects of the nuclear health and safety regulations. The Nuclear and Industrial Safety Agency (NISA) was the premiere agency tasked with being the premier nuclear safety regulatory body. However, the body did not have a significant deal of autonomy as it had to report to and receive recommendations from the Minister of METI and the Cabinet Office (Nuclear Safety Commission). Apart from the Ministry of Economy, Trade and Industry (METI), the Ministry of Education, Culture, Sports, Science and Technology (MEXT) also had the responsibility of oversight of radiation protection and nuclear materials safeguards. Other important bodies and organisations also included in the frame work like the Japan Nuclear Energy Safety Organization (JNES), Nuclear Safety Commission (NSC) and Japan Atomic Energy Agency (JAEA). The regulatory responsibilities provided to the NISA were over but the structure as can be seen from Appendix B is very convoluted which restricted the operational efficiency of the body. This is one of the prime concerns that could be highlighted after the review of the relevant legislation and regulations.
Discussion
TSPF (2012) report offered recommendations across a variety of sections including government wide, legislation wide and on private-public partnerships. The report (ibid.) highlights the need for an authoritative nation-wide chain of command system for managing similar disasters in the future. This can also alleviate the issues of organisation highlighted by Ramachadran & Karthikevan (2014). This organisational change can also be a solution to the resilience crisis in disaster management structure identified by Funabashi and Kitazawa (2012). In this regard the recommendation for a centralised chain of command structure headed by a more authoritative organisation like the NISA could be a perfect solution for the situation from a preparatory and organisational stand point. The TSPF (2012) also notes the role of clarifying the roles of organisational and personnel in such events in a more effective manner so as to reduce the chaos that was observed following the crisis. The report also mentions the development of specific “crisis-response laws” to be able to better empower the responders in the event of another crisis. Preparedness is another aspect that has been highlighted by a lot of the authors ad report published. TSPF (2012) focus on the need to further improve the documentation and training process to be able to assess risks better. Similar recommendations were also forwarded by Ramachadran & Karthikevan (2014) who suggested that risk assessment and risk communication is a key to the degree of preparedness for the plant. Funabashi and Kitazawa (2012) however, highlight the need for more comprehensive critical evaluation of plans and highlight the risk posed as a result of perceived technological perfection. This becomes a critical point because the dangers of dependency of past learnings and omission of proper risk assessment in this specific case led to the underestimation with regards to the dual impact of the earthquake and the tsunami in this case. Therefore, in the opinion of this author, the proper risk assessment, management and communication is critical to the disaster prevention and management. From the evacuation and rehabilitation management perspective as well there were several issues highlighted in the academic writings (Hasegawa, et al., 2016; IAEA, 2014; TSPF, 2012). The main issue identified and recommended for rectification in each of them remained the same – the need for clarification of roles and responsibilities and the need for better structure. In that regard the structural changes recommended in TSPF (2012) if extended judiciously and effectively can be used to create a centralised response apparatus that can effectively communicate with the public and the emergency responders and enable the provision of proper resources at critical times.
Conclusion
The Fukushima Disaster, as it is called happened on the 11th of March 2011 when an earthquake, registering 9.0 on the Richter scale, off the coast of Japan caused a tsunami that hit the Tohoku region of Northern Japan. This caused nuclear meltdowns and hydrogen explosions in the plant and led to the release of radioactive materials into the environment. The event resulted in several physical and mental health consequences for those affected and have been presented in the report. The alarming finding through this research is that radiation exposure did not cause a single death in the event and the scope of damage relating to this event occurred in the management and transportation of people from the evacuation area under untenable circumstances. There were also long term psychological and behavioural issues identified among those affected and evacuated from the region. One of the preliminary shortcomings identified in the report I that of organisational uncertainty and lack of clarity in roles. Based on the evaluation of the recommendations, it is clear that better approaches to risk assessment, design and development, risk communication, disaster response communication and coordination is required to reduce the risks associated with future events like these.
References
Funabashi, Y. & Kitazawa, K. 2012. Fukushima in review: A complex disaster, a disastrous response. Bulletin of the Atomic Scientists, vol. 68, no. 2, pp. 9-21.
Haegawa, A., Ohira, T., Maeda, M., Yasumura, S. & Tanigawa, K. 2016. Emergency Responses and Health Consequences after the Fukushima Accident; Evacuation and Relocation. Clinical Oncology, vol. 28, pp. 237-244.
Hollnagel E. & Fujita, Y. 2012. The Fukushima Disaster – Systemic Failures as the Lack of Resilience. Nuclear Engineering and Technology, vol. 45, no. 1, pp. 13-20.
International Atomic Energy Agency 2014. The Fukushima Daiichi Accident: Report by the Director General.
The Sasakawa Peace Foundation 2012. The Fukushima Nuclear Accident and Crisis Management.
Appendices
A: The legislative and regulatory framework for health and safety in nuclear installations in Japan during the event

B: Position of NISA within the governmental and regulatory framework
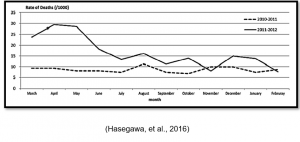
C: Comparison of mortality rates in 2011-2012 to the preceding year
________________________________________________________________________________
Know more about UniqueSubmission’s other writing services:
