
Case Analysis
Compare and contrast of the NASA Challenger and Columbia Disaster
The tenth mission of the American spacecraft mission came to an end with the NASA shuttle obiter Challenger disaster. The space shuttle broke up exactly after 73.6215 seconds after liftoff at 11:39 am on 28th January 1986. The NASA Challenger was hugely publicised and received media coverage as seven crew members including a civilian teacher lost lives in the explosion on board due to the technical fault. On investigation the disaster by a special commission, it was identified that rubber O-rings that isolate the sections of shuttle rocket booster failed to function to seal the joints of solid rocket boosters due to cold temperature (Jenab et al., 2015). This led to hot combustion gases to flames in the booster which due to failed rubber O-rings leaked out and damaged the fuel tank (external) that caused the disintegration of the spacecraft. This tragic disaster pressurised National Aeronautics and Space Administration (NASA) to momentarily suspend its future spacecraft mission.
A similar tragic disaster happened in American spacecraft mission history on 1st February 2003 recognised as Columbia disaster that disintegrated killing seven of the crew members aboard before the scheduled landing at Kennedy Space Center. The disaster happened due to the problem of a foam insulation strike that fell from the bipod ramp (a structure that attaches the shuttle to the external tank) and strikes the left wing of the space craft (Jenab et al., 2015). This breach of wing formed a hole letting atmospheric gases into the shuttle damaging the sensors leading to the tragedy.

From the above spacecraft disasters, it can be noted that apart from the technical faulty, engineers’ awareness and assessment issue there was the lack of adequate communication among the different layers of NASA management. In the case of Columbia disaster, the decision made by the NASA discloses the crew members of Columbia were not aware of the damage and the vulnerable space shuttle during the re-entry. The management of NASA decided that the Columbia crew should not be communicated with the knowledge about the risk. In the case of Challenger disaster, the poor management is reflected as NASA had no proper experience in launching the space craft in cold temperature conditions. According to Weick and Sutcliffe (2011), the coldest temperature the NASA has experienced was 20 degrees warmer during the previous spacecraft launch. Fry (2012) mentions that the rubbers O-rings were not tested prior to launch for functioning in cold temperature conditions. Moreover, Hall (2016) point the culture of NASA is also equal contributor toward the tragic disaster of Challenger and Colombia space mission. Morton Thiokol who was responsible to design and build the solid rocket boosters (SRB) was well aware of the cold –weather problem and project engineers briefed the problem of O-ring seating and joint rotation to the management, but management did not support the re-designing of the task force. The decision making process for the Challenger mission was inadequate as the risk associated with the launch of Challenger space shuttle were known to the designer and builder of solid rocket boosters, Morton Thiokol along with the project managers and the NASA management (Garrett, 2017). The failure of solid rocket booster highlights the poor decision making process by the NASA management. Also, the poorly communicated launch problems by the designer and engineers to the managers and the ignorance of the engineer concerns by the NASA management exhibit the inaptness of the decisions. Another decision taken by the engineers to continue to launch decision in the condition of insufficient low temperature conditions also demonstrate the inadequate decision–making (Robert Mitchell et al., 2011). Similarly, in the Columbia disaster, the problem of foam was well known to the engineers and prior to launch four meetings were held to brief the issue to the management (Boin & Fishbacher-Smith, 2011).
Thus, the two disasters have many similarities in the history of NASA space mission, but there are some major contrasts between the Challenger and Columbia disaster. The exact cause of Challenger disaster was technical failure of rubber O-ring which failed to seal causing solid booster rockets to leak, However, to find the cause of the explosion of Columbia space shuttle was much difficult as the disintegration was not during airlift as in challenger but during the re-entry to Earth orbit after 15 successful days in space. The Columbia disaster which occurred seventeen years later after the Challenger disaster was not due to consequences of individual actions or negligence and breach of safety laws but is related to the culture of the organisation (Edmondson, 2011). A key difference in the culture of NASA that emphasis the safety aspects and open communication policy. During the Challenger disaster, the official at NASA was not much open and responsive to the whole situation but the second disaster the NASA officials exhibit a transformed behaviour and management response Columbia disaster was well handled. The management did not keep the information undisclosed and did not refuse to comment as in the case of first in-flight tragedy(Jenab et al., 2015). The NASA administrator came upfront at that time of the second disaster and assured public the about the investigation that would be highly systematic and discussed the risk and life danger associated with the space mission (Travel, 2014). In Challenger disaster, the important information remained undisclosed to the top management like the Level I and Level II managers and withheld the important information from the community. It can be observed that the Challenger disaster demonstrate a case of a crisis communication failure leading to organisation failure.
The management ignored the concerns of the engineers, and no decisions were taken in these meetings. It can be noted that the launch of these space shuttles was not delayed or halted due to the technical issues raised by the engineers. The management of NASA was keen to launch the Challenger spacecraft for the political pressure, economic consideration and due to several delays in scheduling the Challenger mission due to mechanical reasons (hatch locking mechanism) and weather challenges (Weick and Sutcliffe, 2011). In contrast to this, the Colombia shuttle launch was more inclined towards the political and budgetary considerations.
The organisational structure of NASA is contributing factor to the poor decision making by the managers. There is no alignment of the organisation structure with the technology in NASA. The technologies adopted by the organisation demands the human resources to align the structure of the organisation to be more flexible in nature. A bureaucratic nature is seen in the organisation with a presence of mechanical hierarchy in the structure of NASA (Kwak and Anbari, 2012). In such organisational structure, during the uncertain situation or complex situation the information is not well understood and received which pose a negative implication on the execution of the task in such circumstances. The organisation demands flexibility in the situation where the complexity and uncertainty associated with the technology are high (Reichert and Weber, 2012). An intense level of carefulness is required for the workforce along with enhanced communication, and a higher degree of professionalism is necessary. In organisations like NASA with high technologies, the processing of information needs to be faster to define problems and to set regulations or processes. This is achieved by open communication and work collaboration among different departments to reduce doubts regarding the critical information required to make correct decisions (Dima and Vlăduţescu, 2012). The rigid organisational structure posed a barrier to effective communication between the engineers and the top managers, and the outcome was poor decision making by these managers.
Both the tragic disasters point to the shortcomings in the decision making the process by the management of NASA. The decision making process chain includes different stages where the managers at Level I and Level II are top decision makers at NASA. Due to this structural chain in decision making, the engineering team and the designer were not able to voice the concerns of the Level II or Level II managers to influence the decision regarding the approval of launch decisions.
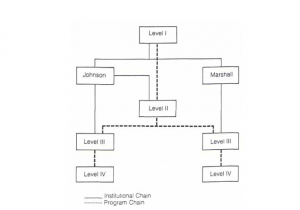
Figure 1 Decision Making Chain Structure for Shuttle Management
(Project Management Institute, Inc., 2017)
These disasters highlight the similar decision-making process by the managers who consider only a few reasons for the launch of these space shuttles and do not take account of the technical issue prior to launch. The problem of rubber O-rings in the rocket boosters was known to the engineers and safety reliability and quality assurance department for the NASA, but the problem was not resolved in the history of the organisation (Safie and Fuller, 2012). The ignorance of the technical problem was to launch the shuttle under the technical problem, and cold weather condition was the biggest flaw in the decision making the process of the management that lead to the in-flight accident. There was no prior examination of the solid rocket boosters, or no alternatives were thought about the foam issues as the engineers were well aware of these problems. Moreover, the decision process by the NASA management rejected the opinion of the experts like project engineers and the designer of the rocket boosters who were against the launch of Challenger space shuttle. The management ignored the negative information related to the launch of the space shuttle and convinced others to view the information which supports the launch on the scheduled day (Robert Mitchell et al., 2011). Also, there was no contingency plan still the decision was taken to launch these space shuttle which resulted in causalities. Furthermore, in both these disasters, few individuals were aware of the problems associated with the launch but failed to brief and communicate properly the issues to the decision maker. This is due to lack of proper communication system lead to flawed decision making process. This demonstrate that the decisions made by NASA demonstrate a poor decision making process which led to the failure of both Challenger and Colombia mission.
Lessons to NASA from the two disasters
After the Challenger disaster, NASA had taken initiatives to improve the safety features and efficiency of the system operations by assigning United Space Alliance (aerospace contractors) for shuttle operational programs (Chicago Tribune, 2017). In the Columbia space shuttle, the O-ring problem was considered, the main engines were reinstated and regularly upgraded, and every part of the system was tested prior to the launch to ensure the safety aspects. Thus, the launch conditions were checked in accordance with the safety parameters and the weather conditions. After the tragic loss of the Challenger mission, NASA made a policy to continuously evaluate the danger to life and risk assessment for each upcoming mission. The investigation team had the advantage to discover and explore the Challenger tragedy as the engine of the rockets and spacecraft pieces were successfully recovered. It was estimated by the National Academy of Sciences the risk or chances of complete space shuttle flight failure is 1 in 145 and in most uncertainty, it can be 1 in 100 (Chicago Tribune, 2017).
The sequence of disaster from Challenger tragedy to Columbia provides a lesson to the NASA management about the ethics of engineering. One of the important considerations under the engineering ethics is to provide necessary tools to the engineers to behave in an ethical way to choose right decisions. The ethical behaviour would be helpful to encourage the engineers to act in a way that prevents any uncertain situation or severe accidents to take place arising from the decisions or action taken by the engineers (Robert Mitchell et al., 2011) . The challenger explosion tragedy is a lesson to be learnt for the engineers and aeronautical staff to behave ethically in professional capacity.
The other lessons that NASA had learned from the Challenger disaster are to develop a culture of open communication and to have in place a proper management control process. NASA provides assurance to redesign the flawed rockets and to develop proper safety mechanism. However, it can be stated that after the Columbia explosion it was clear that NASA has not implemented the changes assured from the first in-flight disaster. According to Donahue and O’Leary (2012), investigation commission mentions that the safety disciplines by NASA management seem to be on paper only for Columbia disaster. NASA had not learned from the disaster to have proper space policies and to break the informal chain of command present in the organisation culture to build a culture that promotes open communication. The redesigning of the foam structure in the rockets and safety mechanism were not implemented that lead to another tragic disaster. The decisions were found to be inappropriate as there were no actions taken regarding the space policies and to deal with the technical issues (Norman, 2011). Moreover, there was no clear communication among the engineers and the upper and middle management. The mangers do not consider different ways to look at the potential issues affecting the launch activities.
Determining factors in the Trull and Bay Area Studies for assessments of strategic decision failure for the two disasters
Strategic decisions are an important outcome for the managerial undertaking in strategic management (Robert Mitchell et al., 2011). Organisational culture plays an important role in shaping the strategic decisions taken by the managers. The managers in an organisation can become less distress to the stressful condition due to culture influence in an organisation. Similarly, Lee et al., (2012) specifies that the engineers in NASA working in the flawed culture of the organisation have become less sensitive towards the likelihood of hazards in dealing with uncertain situations or risky circumstances. This opinion is formed by the investigators of the disasters from Challenger to Columbia that the internal factors of organisation and culture aspects of NASA are pointed to be responsible for the second in-flight disaster.
The determining factors in the Trull and Bay Area studies are vital to recognise the effectiveness of the decisions for the organisation. The effectiveness of decision made by the senior managers is required to be assessed to deal with future consequences (Lunenburg, 2011). In the two space shuttle NASA disasters, the effectiveness of decisions making process is hampered due to the organisational culture and ignorance of the management to technical issues. The Trull and Bay Area studies establish the variables that revolve around the quality and appropriateness of the decision taken by the management. Some determining factors are the compatibility, optimal time for the decision, and closeness of the decision to information, the influence of the problem solver on the decisions and decision implementation by the decision makers (Nielsen and Nielsen, 2011). The strategic decision failure in these disasters is an outcome of poor briefing of the problems by the engineers to the management. The decision taken by the mission management team for the launch of the space shuttles was not compatible with the existing conditions which were the technical issue in both cases and additionally cold weather in the Challenger launch. The time taken for the decision by the manager not to delay the launch schedule due to problems was not near to the information provided by the engineers. It was also observed that the decision makers like the upper managers of NASA have influence over the engineers and related concerns resulting in the decision to launch these space shuttles. The managers ignored the negative information and safety policies and focused on only the commercial consideration to be gained from the launch.
The factors such as autonomy and interdependence in an organisation are known to hinder the effectiveness of the regulator bodies to prevent the occurrence of disasters and accidents. According to Benson and Voller (2014), autonomy is the complexity in obtaining information from a business unit or organisation that is present autonomously of the information seeker. In autonomy, the regulator develops an interpersonal relationship with others to gather information for better understanding. Interdependence refers to the dependence of one business on other business units for the success and failure (Reichert and Weber, 2012). The interdependence factor has a large influence on the regulator who might not force significant approval on other business units or operations. In the case of NASA, there was one external regulator who did not follow the technical problem of O-rings. At the same time, the two internal regulators were well aware of the problem related to the official launch of the space shuttle. Even the department of safety, reliability and quality assurance was fully aware of the technical issue, but the department lacks the knowledge about the engineers briefing of the problem and objection related to the launch of Challenger space shuttle. Thus, this lack of participation is an indicator of the autonomy problems in the NASA. The factor of interdependence is associated with the restrained approval is another cause of the problem in the NASA management (Benson and Voller, 2014). The ignorance of launch problems and no serious solutions to these problems by the managers at a higher level is an indicator of interdependence issue in NASA.
Furthermore, the decisions taken after the Challenger disaster were not implemented by the organization leading to the decision failure in Columbia disaster. According to Kalali et al. (2011), the decision is put into organisational practice are influenced by the prevention of conflict of interest, the extent to which the understanding of information for the decision is achieved and the factors related to rewards and risk associated with the implementation of the decision. The strategic decision failure for the two disasters highlight that the decision and lessons learnt from the first in-flight tragedy was not implemented in the NASA culture as the management failed to measure the risk associated with exemption of the space policies, bureaucratic structure with informal chain of command.
Recommendation for the NASA management
Observing both the disasters, it can be suggested that the space shuttle should design and set policies to design a launch escape plan or system to assist the crew members on board to make aware of the safety issue during the breakup and to avoid negligence of the safety parameters to avoid such disasters. The management of NASA is required to have contingency plans prior to launch (Dyke et al., 2011). Some formal rules are required to be present within the organization to handle the unexpected event effectively and efficiently to reduce the impact arising from unexpected outcomes. Garud et al. (2011) found that there was inherent vagueness in the work of NASA engineers in relation to the identifying the precautionary steps for the hazard identification. In the ethics of engineers, it is significant to understand the responsibility associated with the engineering profession to act towards prevention of hazards (Harris Jr et al., 2013). Thus, it is suggested to the NASA management to have an organised system of assigning responsibility to each mission management team including project engineers and designers to develop a high level of ethical behaviour. By developing engineering ethics and a sense of ethical behaviour towards the profession and assigned responsibility would be an appropriate way for the NASA to prevent such tragic disaster in future space missions. Improvement in culture and ethical practices would also be useful to reduce the likelihood of hazard in the system that is of the complex technological structure (Kalali et al., 2011).
Besides, the management should have a formal chain of command and open communication policy to achieve the process of the strategic decision for its future missions. Improving communication process within the NASA culture is essential to deal with the structural flaw of the organisation which is complex and bureaucratic in nature (Space Safety Magazine, 2014). Effective communication would lead to an open exchange of necessary information regarding the safety matters, and it would provide an opportunity to the management to evaluate the engineer’s concerns about the shuttle launch. The presence of formalised decision support system in the organisation would be effective to fulfil the requirement of safety aspects and would encourage the participation of the regulators in the pre-launch process of decision making (Barnabè, 2011). It is also recommended for NASA to incorporate training programs for the mission team to identify the ongoing issue prior to the launch in accordance with the available resources. It is also vital for the organisation to implement regular inspection of the structural integrity of the panels, hardware and supporting structure and should have flexibility for flight schedule in case of uncertainties. There is a need for the management of NASA to re-consider its organisational structure and its alignment with the organisational strategy. The organisation should also integrate the flexible structure with the business objectives, space mission goals with the needs of the human resources (Barnabè, 2011). An integrated decision support system is useful for the managers to get accurate information for the key decision makers and to respond to issue proactively. It is also essential for the organisation to align its technology with the required flexible organisation structure. This would lead to effective decision making and holds relevance to strike a balance with the organisational structure, goals, training, technology, social commitments, and the external environmental factors.
References
Barnabè, F. (2011) A “system dynamics-based Balanced Scorecard” to support strategic decision making: Insights from a case study. International Journal of Productivity and Performance Management, 60(5), pp. 446-473.
Benson, P. and Voller, P. (2014) Autonomy and independence in language learning. United Kingdom: Routledge.
Boin, A., & Fishbacher-Smith, D. (2011). The importance of failure theories in assessing crisis management: The Columbia space shuttle disaster revisited.Policy and Society, 30(2), 77-87.
Chicago tribune. (2017) Key differences seen in Columbia, Challenger disasters. [Online] Available at: http://www.chicagotribune.com/news/nationworld/chi-0302020335feb02-story.html (Accessed: 27 May 2017).
Dima, I. C. and Vlăduţescu, Ş. (2012) Risk elements in communicating the managerial decisions. European Journal of Business and Social Sciences,6(1), pp. 27-33.
Donahue, A. K. and O’Leary, R. (2012) Do shocks change organizations? The case of NASA. Journal of Public Administration Research and Theory, 22(3), pp. 395-425.
Dyke, G., Gill, S., Davies, R., Betorz, F., Andalsvik, Y., Cackler, J., & Lamboglia, E. (2011) Dream project: Applications of earth observations to disaster risk management. Acta Astronautica, 68(1), pp. 301-315.
Edmondson, A. C. (2011) Strategies for learning from failure. Harvard business review, 89(4), pp. 48-55.
Fry, E. K. (2012) The risks and impacts of space weather: Policy recommendations and initiatives. Space Policy, 28(3), pp. 180-184.
Garrett, T. M. (2017) Katrina, Rita, Challenger and Columbia: Operationalizing a Knowledge Analytic in NASA and DHS Crises. Public Voices, 10(1), pp. 23-35.
Garud, R., Dunbar, R. L. and Bartel, C. A. (2011) Dealing with unusual experiences: A narrative perspective on organizational learning. Organization Science, 22(3), pp. 587-601.
Hall, J. L. (2016) Columbia and Challenger: organizational failure at NASA.Space Policy, 37, pp. 127-133.
Harris Jr, C. E., Pritchard, M. S., Rabins, M. J., James, R. and Englehardt, E. (2013) Engineering ethics: Concepts and cases. United States: Cengage Learning.
Jenab, K., Khoury, S., Fine, T. and Moslehpour, S. (2015) Cause-Consequence analysis for NASA’s space transportation system (STS)-solid rocket booster (SRB). International Journal of Business and Management,10(8), pp. 23.
Kalali, N. S., Anvari, M. R. A. and Dastjerdi, A. A. P. D. K. (2011) Why does strategic plans implementation fail? A study in the health service sector of Iran. African Journal of Business Management, 5(23), pp. 9831.
Kwak, Y. H. and Anbari, F. T. (2012) History, practices, and future of earned value management in government: Perspectives from NASA. Project Management Journal, 43(1), pp. 77-90.
Lee, S. M., Olson, D. L. and Trimi, S. (2012) Co-innovation: convergenomics, collaboration, and co-creation for organizational values. Management Decision, 50(5), pp. 817-831.
Lunenburg, F. C. (2011) Decision making in organizations. International journal of management, business and administration, 15(1), pp. 1-9.
Nielsen, B. B. and Nielsen, S. (2011) The role of top management team international orientation in international strategic decision-making: The choice of foreign entry mode. Journal of World Business, 46(2), pp. 185-193.
Norman, G. (2011) Chaos, complexity and complicatedness: lessons from rocket science. Medical education, 45(6), pp. 549-559.
Project Management Institute, Inc. (2017) The Space Shuttle Challenger incident. [Online] Available at: https://www.pmi.org/learning/library/lessons-space-shuttle-challenger-incident-5243 (Accessed: 25 May 2017).
Reichert, M. and Weber, B. (2012) Enabling flexibility in process-aware information systems: challenges, methods, technologies. USA: Springer Science & Business Media.
Robert Mitchell, J., Shepherd, D. A. and Sharfman, M. P. (2011) Erratic strategic decisions: when and why managers are inconsistent in strategic decision making. Strategic Management Journal, 32(7), pp. 683-704.
Safie, F. M. and Fuller, R. P. (2012) NASA applications and lessons learned in reliability engineering. In Reliability and Maintainability Symposium (RAMS), 2012 Proceedings-Annual (pp. 1-5). IEEE.
Space Safety Magazine. (2014) The Space Shuttle Columbia Disaster. [Online] Available at: http://www.spacesafetymagazine.com/space-disasters/columbia-disaster/ (Accessed: 25 May 2017).
Travel, T. C. S. (2014). Fatality Risks on the Road and in Space. The American journal of medicine, 127(6).
Weick, K. E. and Sutcliffe, K. M. (2011) Managing the unexpected: Resilient performance in an age of uncertainty (Vol. 8). USA: John Wiley & Sons.
