DEN763 Advanced General Dental Practice Assignment Sample
Here’s the best sample of DEN763 Advanced General Dental Practice Assignment.
Part A
Demonstration of Knowledge and Understanding
Dental Bonding or adhesive agents comprise a complex chemical, physical and mechanical mechanism which allows the attachment of substances. This can be defined as a material that has a lower viscosity, while applied on the surface of teeth and a thin film is formed after setting with teeth. This film is strongly bonded to the surface of the teeth on which the viscous compound restorative resin is applied. An integrated resin is restored and formed. Resistance to the separation of an adherent is provided, Stress distribution along the bonded interface is distributed, Reduce microleakage and seals the interference through the adhesive bandings; these are the main functions that are carried out by dental bondings. According to the history of dental bonding, Castan developed an epoxy molecule in 1938. This is a molecule that is made up of one oxygen that is bonded with two carbon atoms which is a Novel crystalline nano composition called epoxy resin applied in esthetic density (Collares et al 2017). After that in 1951 “glycerophosphoric acid dimethacrylate” was developed by Dr Oscar Haggart which is used as a cavity sealer. “Acid etching technique with phosphoric acid” was introduced by Buonocore in 1955 and in 1956 the first dentin bonding agent was introduced. After that in 1957 “BIS GMA” resin system was introduced by Bowen. This resin is used in the dental composite, dental cement and as dental sealants. This is a diester molecule that is derived from The acid methyl acrylate and the diglycidyl ether named bisphenol. In 1965 the working principle of primers was described by Causton. The pattern of etching of enamel is described by Gwinnett and Silver stone in 1975. This invention process is carried out with different inventions until 2003 the 7th generation of bonding agent was developed by Ferrari.
There are different generations of evolution involved to develop the bonding agents in Dentistry. Choosing a dental adhesive agent is a need to balance the ease of use, strength, efficiency and techniques. The efficiency of the adhesins totally depends on which generation agent is used. There is a total-etch system in the fourth generation and a no-etch system in the fifth generation. The sixth-generation provides self-teaching advancement. The evolutionary study of bonding is needed to know the advancements that are offered by different generations and what they offer in practice. There are a total of eight generations that are involved in the evolution of dental bonding agents. Here is the study of different generations are briefly described-
First Generation:

Those debuted in the year 1950. Dr Michael Buonocore identified a deficiency of tooth adhesive substances that acts as a major lacking in failure of the restoration. In 1955 the use of acid etching for the bonding purpose was proposed by him (Essam 2018). This demonstrates a resin that is containing a chemical agent named “NPG-GMA” that could bond the “acid-etched dentin” that improves the adhesion of filling materials to enamel-1. This became unsuccessful due to the reduction in the mouth due to the moist environment inside. That leads to the innovation of second-generation improvement.
Second Generation:
Polymerized phosphates were added with the “Bis-GMA” resin that increases the strength of bonds and that is mediated by an ionic bond to the calcium of the tooth. A smear layer was not found at that time, that’s why unreliable bond strength was produced. Though the small improvements take place but still the bonds are not so stable they degrade quickly. Until the smear layer was addressed the evolution could only be minimal. In the late 1970s, the smear layer and its effect on bonds were identified by Dr David Eick.
Third generation:
In the 1970s and 80s, smear layer removal became an important goal of the bonding technique. The acid etching is used to remove the inorganic or organic coatings during the preparation of the cavity. This introduction of the new technique is not received by all dentists that are why it became controversial, as many dentists thought that dentin should not be etched. While acid etching is served to open the tubules of dentin and which allow the removal of the smear layer particles more efficiently. After rinsing the acid primer was applied and then to the dentin and enamel infill resin was placed. There are many problems that remain unsolved in this generation and that leads to the third generation.
Fourth generation:
This generation changes the bonding game permanently. The researchers finally found a way to efficiently remove the smear layer. There are numerous application steps that are involved in this process. The efficiency of this generation made them long-lasting and stand by for many dentists (Gesko et al 2017). The familiar names “OptiBond”, “Clear Fi”, “BISCO” emerged and forerunners of products are commonly used today. According to Dr Nathaniel Lawson, “The adhesive materials with the longest evidence of clinical success are definitely the two-bottle systems—either the fourth-generation etch-and-rinse materials or the sixth-generation self-etch materials”.
Fifth-generation:
The conquered smear layer and the improvement in the bond strength that is improved in the fourth generation, the goal of the fifth-generation became the simplification of the system of procedural and time management and the sensitivity of the post-operation. The fifth-generation came with the one bottle system that combines the primer and the adhesive in a single bottle. That made this able to apply to the enamel and dentin consequently. But the drawbacks came along with simplicity: not all the adhesives of this generation are used with dual or self-cure materials. This system also contains the primer which is hydrophilic in nature that makes the adhesives much more liable to degradation in moisture. Despite these lickings, the one bottle system was received by clinicians, it reduced the chair time and reduced the need to stock multiple adhesives and primers.
Sixth generation:
Self-etching bonding agents were founded in this generation. They did not require phosphoric acid to dematerialize the tooth. They include self-etching primers that dematerialize and also prime the tooth simultaneously (Innes et al 2020). Hydrophobic adhesives are also utilized that make a bond more readily. In type 1 Self-etching the primer and the adhesives are applied in two different steps whereas in type 2 those are mixed together that’s why They are mixed and immediately applied within a single step. “One coat self-etchingBond” is an example of a Sixth generation type 1 product.
Seventh generation:
The seventh-generation bonding agents are used to bond the composite materials reliably to the enamel and dentin. This generation bonding is among the best bonding systems mainly that improve the bonding agents that have resulted in some components with fewer steps and with better predictability in the practical area.
Universal generation:
In the year of 2010 “VOCO America” introduced this last generation bonding agent. This is an all in a one-step process that limits the number of bottles and reduces the clinical time. The nano-size filler is used in this generation. This has dimensions larger than 15 to 20 nm that may cause the crack and may decrease the bond strength that’s why 12 nm filters are used. The use of these “Nano-size fillers” that increase the resin monomer penetration and the thickness of the hybrid layer will be discussed. That also improves the bonding system mechanical property.
The improvements in each generation open new doors in the bonding system.
Cognitive, Analytical and Evaluation Skills:
Critical thinking and reasoning:
Critical thinking is the process that involves improvement. Dental and the students of dental hygiene can be benefited from the reflective thinking that helps them to make reasonable decisions about their patients. Along with this skill, clinical reasoning skills should be needed to be developed. For patient’s data assessment, clinical reasoning skill is applied. This continues through the development and implementation of the care plan. This continues through the evaluation of the effectiveness of the plans and current documentation of the patient care.
The Paul-Elder Critical Thinking Framework:
Another of the objectives of dentist school is to stimulate, improve, and fortify students’ critical reasoning skills. The concept could also be used to educate children to think across all academic and practical environments. If one person understands how and when to educate, there is also no limit to the number and type of data that may gain during their lifetime will be discussed. The first level of Cohen’s categorization may well be achieved by rote learning. If a person can merely recollect data, they would indeed fail to develop as personalities or learners, but its connections with patient care will be constrained.
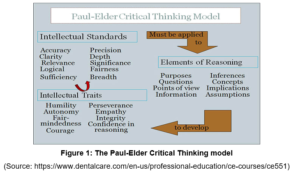
“Paul-Elder Critical Thinking Model” is divided into three aspects. That the very first component seems to be the “Foundations of Thinking,” also referred to as “The Aspects of Mind,” which emphasizes here the structural improvement of mental process. The second part seems to be the “Universal Intellectual Standards,” which can provide methods to evaluate the adequacy of the process of thinking. The third part is “Intellectual characteristics,” which seem to be intellectual patterns that occur as the result of compatibility of the idea of this approach to the different aspects of reason.
Elements of reasoning:
Considering differentiates beyond critical analysis except that it fulfils some conditions that have been opposed to haphazard thoughts. That the very first stage in analytical analysis is really to determine key components of thinking that will permit the problems to just be discovered. If it can do this, then it could resolve problems or go to a broader focus as a serious person, and contain ingredients of argumentation.
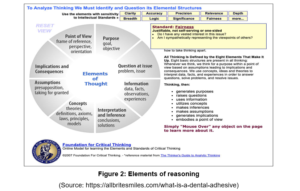
The purpose is clarified about the goal and the objective of the task. The questions that find out the problems and issues, information are collected to know the data, facts and observations and help to gain experience through the task. The information involves all the associated knowledge and information to solve any issue. Concepts are used to develop knowledge about different theories and hypotheses. The point of view clarifies the task or problem. Those are the different elements of reasoning that help to solve any problem critically.
Intellectual Standards:
Another challenge in evaluating personality is matching this to logical criteria. The Paul-Elder framework incorporates eleven methods for evaluating the ability to reason that may have been related to the Foundations of Cognition. And using these principles openly will produce simpler, higher correct, stronger, and so more important thoughts. Among mental qualities are readability, precision, precision, relevancy, breadth, range, reason, meaning, and impartiality.
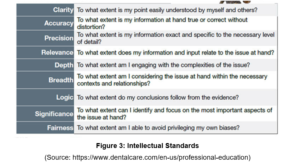
Those nine “Mental Competencies” are resources that a medical hygienist might utilize whenever communicating with patients, peers, and learners. The principles help practitioners and learners to question things or to be the best they can always be.
Application to Clinical Practice
This reflective practice and knowledge are put to use in actual life. The “Paul-Elder model” assists the students in focusing on therapeutic problems. Instructors, for one, may ask the students about inquiries they had around their patients after interacting with individuals. They could question what knowledge will aid physicians in solving their issues, if indeed the information is essential to clinical judgment, as well as what expectations clinicians have of the patient. So when the participant’s perspective is respected, the interaction here between the dental physician and the patient improves, and also the person is far more open to considering treatments and making targets to better their dental health will be necessary. Understanding to connect the guidelines’ specific conceptual parts supports the practitioner in evaluating the value for overall patient’s care. The components of reason led to adjustments in care delivery depending on the risk signs and the participant’s stabilization. The assessment of issues, or the important details and varied conceptions needed to support and help patients, seem to be the most crucial concerns to discuss all throughout the visit.
Part B
Restoration is the way to restore or replace missing teeth or any missing part of the tooth structure or any tooth structure that need to be removed to prevent tooth decay or pain in future. Before the dental restoration teeth should keep clean by flowing or brushing. The dental cavity is treated with filling. There are different restoration techniques used for different damages of teeth and they are, Filling, Crowns, Teeth implants, bridges and dentures.
In this particular case study, The 35 years old woman has caris in the upper right first and second premolar teeth. A dental crown is done by using different dental amalgams and that contain different alloys like silver, tin, copper and mercury up to 10%. There are some drawbacks associated with these amalgam fillings. The presence of mercury is the major factor and other than that, a higher amount of tooth preparation is required for a strong filling and restoration has a dark colour. The patient wants to treat her teeth with amalgam-free cosmetic replacement. There are different filling options available for this treatment such as ceramic filling, and filling with composite resins. The strength and durability of these filling materials and the patient and doctors are now showing more interest in amalgam-free filling.
Restorative treatment deciding factors:
Caries extent
The remaining tooth structural strength
The specific characteristics of dentition and periodontal health
History of patient’s oral health and hygiene
The costing of the procedure
Risks and benefits of the procedure
Ability of clinician to perform the procedure
Dentist preference and prevalence standard care
Patient’s acceptance
Choice of bonding agent to fill the cavity:
The ceramic feeling is chosen to treat the cavity instead of the composite filling. The composite filling is in peril to staining. Those can also lose the polish and become dull than tooth enamel. In contrast, the ceramic filling can resist the stain and can maintain teeth polish. That makes them the better choice for making such a feeling that becomes highly visible after treatment. That’s why the ceramic filling is chosen to fill the cavity of the patient.
Pros and Cons of choosing ceramic filling:
Ceramic is called the filling of porcelain. This does not attach with the teeth as the amalgam fillings. The material covers up the cavity and can shape to perfectly fit the cavity. The material looks like original teeth (Yuan et al 2019). This procedure is more expensive than other available filling procedures. This requires the removal of a greater number of healthy teeth besides the damaged teeth due to the bulky nature of the feeling agent. This needs multiple visits to the clinic before the filling is in place.
To maintain the filling the patient needs to follow proper oral hygiene. Need to visit the dentist after each regular time interval for proper cleaning, fluid brushing or brushing in a conventional way. Using antibacterial mouthwash properly is necessary. The proper check-up of the filling to observe if there are any cracks or not. If the crack is observed then an X-ray is applied to know the situation. If any sharp edge or any issue of sensitivity observed or crack observed in filling or canny piece of filling will be missing, then the patient should contact immediately with the doctor.
Good contact:
Restorative procedures have the primary objective to make an interproximal contact. The ideal proximal contact that acts as a barrier against the impaction of food and thus it contributes to underline the periodontal health and that is by providing hygiene cleaning and the food spillway will be discussed. This is defined as the point when teeth acquire and erupt the contact with adjacent teeth that lead to the conversion of the contract point area. The proximal area of contact or the area of contact is where the surface of the teeth in a neighbour comes in contact. The area is usually located in the upper one-third of the crown area of most teeth. This provides a good opportunity of maintaining the interproximal area of two adjacent teeth. The Premolar teeth of the patient have near proximity in between two teeth that’s why it has a good contact site.
The features of an ideal contact site are:
That maintains the dental arch and stability by the fore transmission along the long axis of the teeth. The proper and correct relationship with the neighbour teeth allows good support against the masticatory forces that promote the deflections of the food particles through the embrasure. That also influences the speech and the cosmetic in the anterior region. The important restoration in the area of contact that causes the displacement of teeth and the teeth lifting force, teeth rotation, occlusal contact and compactness of the food will be discussed.
Self Development:
The problem is that you’ll have all the abilities within the world compared towards becoming a dentist, but if one does not really make the time for individual improvement whilst gaining this expertise, the education could become a pompous scrap of paper. We’re here now to educate students about just the relevance of individual improvement in being a dentist, so one may begin to enjoy operating on mouths rather than just simply getting and through procedures.
Development of personal vs professional
Before you could even discover how and when to begin any self-improvement adventure, everyone should first grasp what it comprises. Professional growth is mainly concerned with personal growth. It’s also about expanding one’s own knowledge, capabilities, and understanding and customizing those to fit who and what one is as a human.
Personal development requires anything one wants to help to develop their abilities, including obtaining a degree or completing a lecture. Nowadays that recognizes the difference, how self-improvement may help one to improve as both dentistries.
The work which has to be done
One will gain more of you as a physician as they go through the coaching and mentoring phase. One will become more informed of their talents along with the ideals and ideas about just this focus on business.
It offers one a better meaning because of what one needs from their work, and one will be able to adjust better targets as a response.
Making clear goals
When we push ourselves, we will indeed be able to clarify targets for what it is we want to accomplish. Thus, if we believe one needs to take the extra school upon anything relating to dentistry after then starting his own clinic, it is Ok. It doesn’t really have to be closely correlated to dentists. Maybe one may get up in the middle of the evening thinking how much that liked the English and Spanish program that one did in university and longing to go somewhere else to acquire additional knowledge. We also get to follow someone you’re engaged in, and then if we improve speaking English, that is indeed actually more people who may benefit through the skill.
Motivation
While one has less distinct objectives, one is more willing to accomplish these. This is especially the case if we write a self-improvement notebook during our journey. There, in a lengthy period, one will become even more effective when this refers to dental surgeon concerns.
Balance of work-life
If users simply go through rituals of washing the mouth, one’ll get dissatisfied with it. If you ever see they heading down that same path, it’s time to step back away and work through your own improvement. By taking a moment to discover more about you and how dentistry, one will find where that genuinely wish to go along with it or one wants to remain to do it again.
Prospects of career
The prime objective of individual improvement is to remove them from their own physician persona. Though this is correct, it may positively enhance overall career opportunities. Because understand, through this consciousness phase, one will understand well how to make oneself prosper (Zurányi et al 2019). If businesses wouldn’t own their own firm, everybody would realize, from normal visitors to their bosses. It could provide them with an opportunity for others in a similar profession.
Out of comfort zone
There’ll be areas of being such a dentist that one should shine at and the others in which you will battle. Spending time for reflection will push one to explore not only his abilities but also potential shortcomings. And while it may force one to venture even outside the personal bubble, it’ll also benefit readers. Until you’re obliged to step back a bit to examine their difficulties, one could stop getting irritated for them and start attempting to fix issues.
Conclusion
It is concluded that according to this case study this patient has the cavity or dental caries in the premolar teeth with the existing large restoration of amalgam in the upper right first and the second teeth. The patient wants amalgam-free cosmetic replacements. In the first premolar, the filling is disto ocular and in the second premolar, the filling is miso ocular. The ocular is stable without any harmful parafunction. A local anaesthetic and rubber dam is applied in this process and the teeth are made free from caries and restorable. The bonding agent is the ceramic filling that is used to fill the cavity of the teeth and there are good contacts in between the teeth that help to proceed with the process of treatment of restoration. There are some measures of concerns among pros and cons that are briefly mentioned through the assessment that needs to be known for the patient while receiving any restoration treatment. “The Paul-Elder Critical Thinking Framework”, “Elements of reasoning” and “Intellectual Standards” are the critical thinking analysis strategies that help the clinician and students to think critically about any problem and analyze them with great solutions by applying them in practical fields.
Reference List
Journals
Collares, K., Opdam, N.J.M., Laske, M., Bronkhorst, E.M., Demarco, F.F., Correa, M.B. and Huysmans, M.C.D.N.J.M., 2017. Longevity of anterior composite restorations in a general dental practice-based network. Journal of dental research, 96(10), pp.1092-1099.
Essam, O., 2018. The Development of the Endodontic Complexity Assessment Tool (E-CAT) for Assessing Endodontic Complexity and Its Prevalence in General Dental Practice. The University of Liverpool (United Kingdom).
Hurst, D. and Greenhalgh, T., 2019. Knowing in general dental practice: Anticipation, constraint, and collective bricolage. Journal of evaluation in clinical practice, 25(6), pp.921-929.
Innes, N.P., Clarkson, J.E., Douglas, G.V., Ryan, V., Wilson, N., Homer, T., Marshman, Z., McColl, E., Vale, L., Robertson, M. and Abouhajar, A., 2020. Child caries management: a randomized controlled trial in dental practice. Journal of dental research, 99(1), pp.36-43.
Innes, N.P., Clarkson, J.E., Douglas, G.V., Ryan, V., Wilson, N., Homer, T., Marshman,
Kersbergen, M.J., Creugers, N.H., Hollaar, V.R. and Laurant, M.G., 2020. Perceptions of interprofessional collaboration in the education of dentists and dental hygienists and the impact on dental practice in the Netherlands: A qualitative study. European Journal of Dental Education, 24(1), pp.145-153.
Kim, J., 2020. What is Dental Advanced Life Support?. The journal of the Korean dental association, 58(10), pp.640-648.
Mills, I.J., 2018. The delivery of person centred care in general dental practice (Doctoral dissertation, Exeter and Plymouth Peninsula Medical School).
O’Toole, S., Khan, M., Patel, A., Patel, N.J., Shah, N., Bartlett, D. and Movahedi, S., 2018. Tooth wear risk assessment and care-planning in general dental practice. British dental journal, 224(5), pp.358-362.
Plessas, A. and Nasser, M., 2019. Can we deliver effective alcohol-related brief advice in general dental practice?. Evidence-based dentistry, 20(3), pp.77-78.
Rosenblum, S., Isett, K.R., Melkers, J., Funkhouser, E., Hicks, D., Gilbert, G.H., Melkers, M.J., McEdward, D., Buchberg-Trejo, M. and National Dental PBRN Collaborative Group, 2021. The association between professional stratification and use of online sources: Evidence from the National Dental Practice-Based Research Network. Journal of Information Science, 47(3), pp.373-386.
Sam, M., Andrews, S. and Eapen, B., 2019. ESSENTIAL HARDWARE FOR MANAGING MEDICAL EMERGENCIESIN A DENTAL CLINIC PRACTICE. INDIAN DENTAL ASSOCIATION THIRUVALLA.
Taylor, G.D., Pearce, K.F. and Vernazza, C.R., 2019. Management of compromised first permanent molars in children: Cross‐Sectional analysis of attitudes of UK general dental practitioners and specialists in paediatric dentistry. International journal of paediatric dentistry, 29(3), pp.267-280.
Teoh, L., Stewart, K., Marino, R. and McCullough, M., 2018. Antibiotic resistance and relevance to general dental practice in Australia. Australian dental journal, 63(4), pp.414-421.
Thanakitprapa, P., Jaratrasamee, A. and Pachimsawat, P., 2017. Autoclave monitoring and packaging in Bangkok dental offices, Thailand. M Dent J, 37, pp.173-82.
Toon, M., Collin, V., Whitehead, P. and Reynolds, L., 2019. An analysis of stress and burnout in UK general dental practitioners: subdimensions and causes. British dental journal, 226(2), pp.125-130.
Yeung, V. and Chandan, J., 2018. The impact of diabetes on treatment in general dental practice. Dental Update, 45(2), pp.120-128.
Yuan, S., Humphris, G., Ross, A., MacPherson, L. and Freeman, R., 2019. Recording communication in primary dental practice: an exploratory study of interactions between dental health professionals, children and parents. British dental journal, 227(10), pp.887-892.
Zurányi, A. and Tóth, Z., 2019. Risk assessment of medication-related osteonecrosis of the jaw in general dental practice. Orvosi hetilap, 160(7), pp.243-251.
________________________________________________________________________________
Know more about UniqueSubmission’s other writing services:
